Sample Preparation
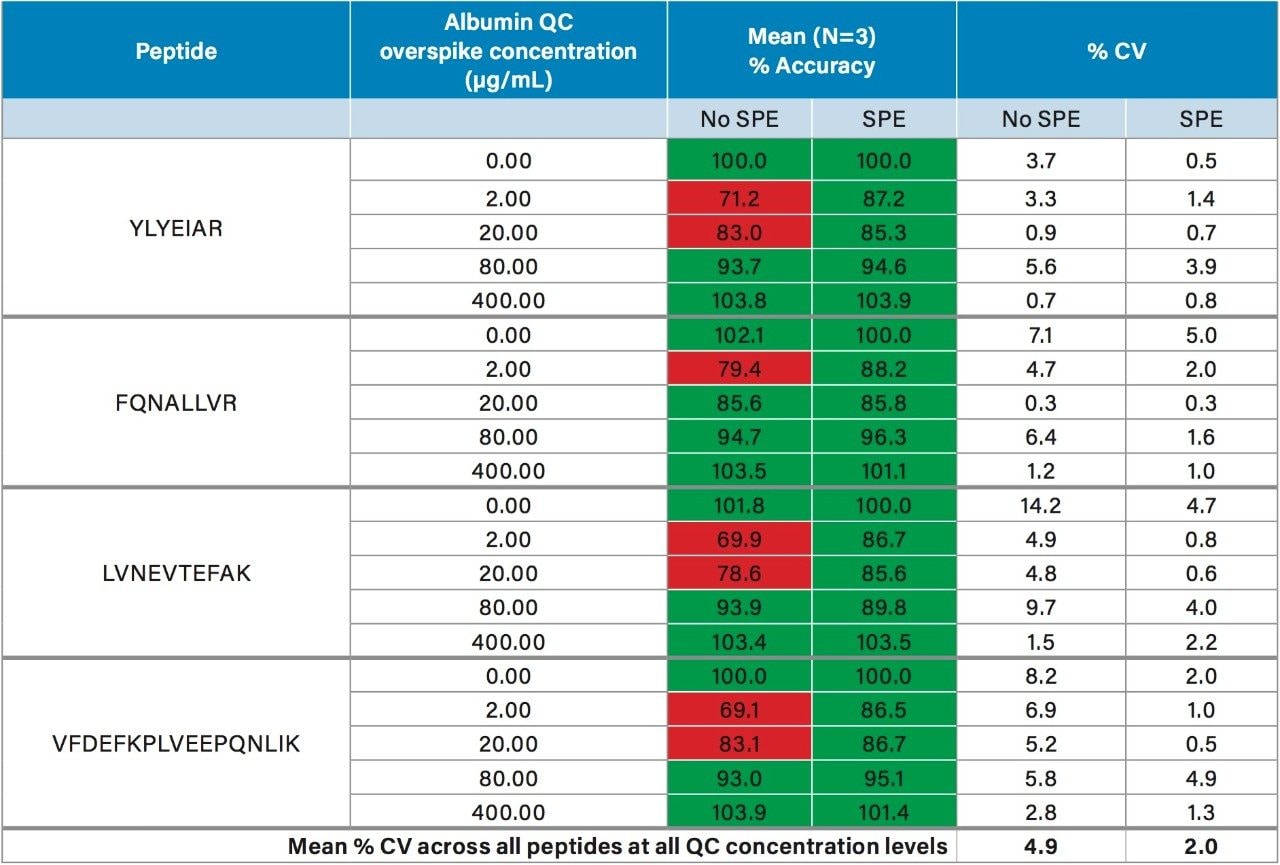
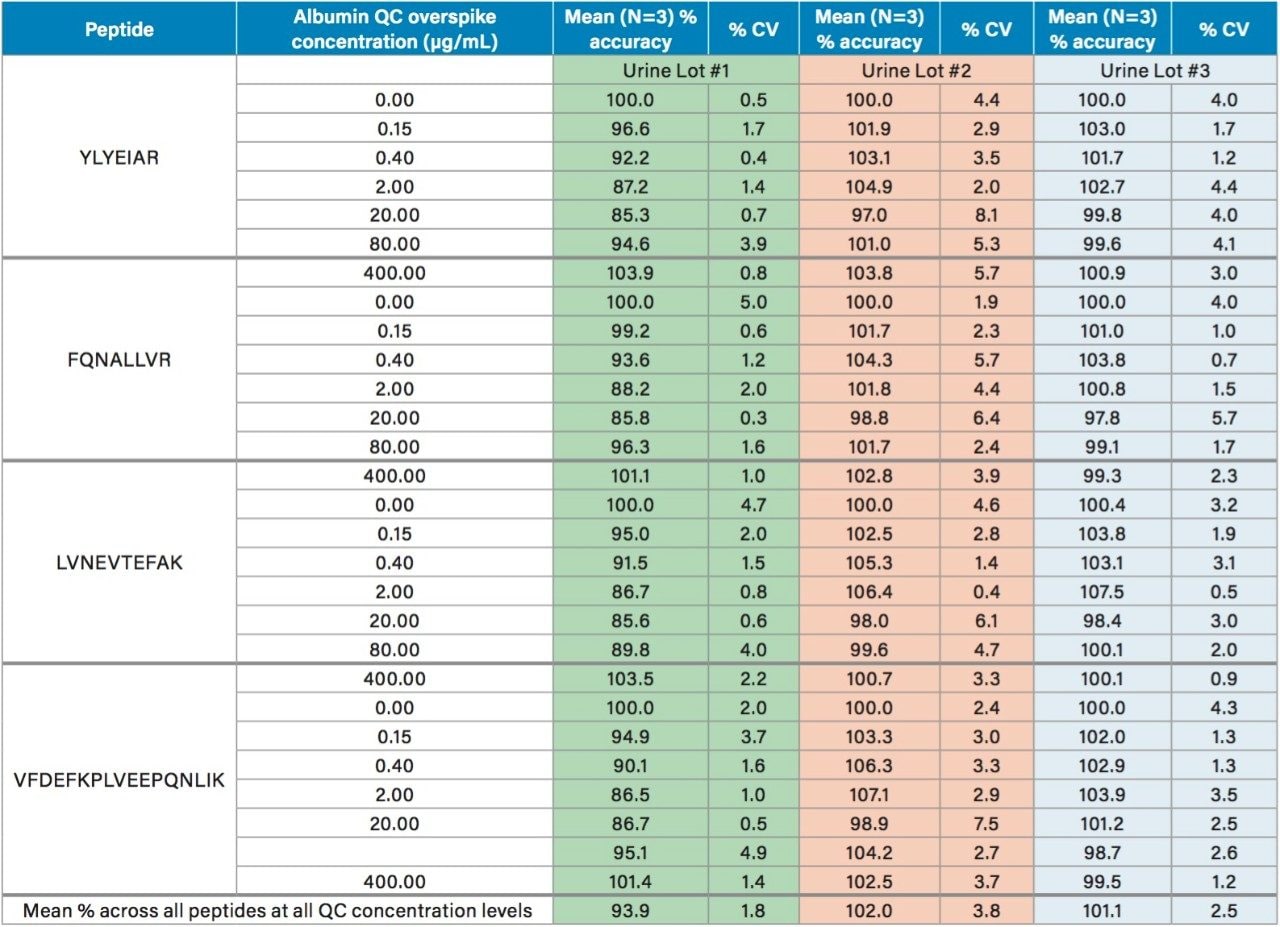
In this work, we used the ProteinWorks eXpress Digest Kit to simplify the quantification of urinary albumin using only 15 µL of sample, and a direct 2-hour digestion (no affinity purification necessary). Specifically, the 5-Step digestion protocol provided with the kit was used. This protocol employs reduction and alkylation to aid in the unfolding of the albumin protein prior to digestion, facilitating efficient enzymatic cleavage. Subsequent purification of the albumin tryptic peptides was achieved with the ProteinWorks µElution SPE Clean-Up Kit, and supplied protocol. This kit contains the mixed-mode sorbent, Oasis MCX, to improve selectivity and analytical sensitivity, effectively removing buffer salts, phospholipids, and excess digestion reagents post digestion, while also concentrating the sample. During method development, quantification of urinary albumin was assessed with and without peptide purification by SPE. While eliminating the SPE step still enabled accurate quantification for the calibration standards (meeting recommended LC-MS method development criteria for linearity, accuracy, and precision13), acceptable accuracy of all QC levels across the various lots of human urine tested could not be achieved without SPE. Comparison of the mean accuracy and precision (%CVs) in urine Lot #1, with and without SPE is highlighted in Table 2. For QC samples prepared without SPE, accuracies across the 4 primary peptides used for quantification failed to achieve the recommended criteria of 85–115% across all concentration levels. Employing a mixed-mode SPE clean-up step significantly improved accuracy and precision of the QCs across all lots of urine tested, easily meeting recommended LC-MS method development criteria. Furthermore, average %CV without SPE was 4.9%, this was improved to 2.0% with SPE. Additionally, the µElution format allowed elution in only 50 µL, providing a 2-fold concentration of the sample, thus further improving detection limits. Traditional protein quantification workflows which employ the bottom up technique are complex and time consuming, often taking >18 hours to complete. Use of the ProteinWorks digestion and SPE kits yielded a total sample preparation time of <4 hours, which allows for same day LC-MS analysis.