A 20 μL aliquot of normal human serum (Gemini Bio, Woodland, CA) was depleted of the six most abundant proteins: Top6 (albumin, IgG, anti-trypsin, IgA, transferrin and haptoglobulin) according to manufacturer’s specifications (Agilent, Palo Alto, CA). Another serum aliquot (80 μL) was depleted of twenty high abundance proteins: Top20 (albumin, IgGs, transferrin, anti-trypsin, fibrinogen, haptoglobin, acid-1 glycoprotein, plasminogen, a-2-macroglobulin, ceruloplasmin, apolipoproteins A1, A2, B, and complement C1, C3, and C4) using a ProteoPrep imuno-depletion cartridge (Sigma- Aldrich, St. Louis, MO).
Serum samples were denatured in 0.1% RapiGest reduced with 5 mM DTT, alkylated with 10 mM IA and digested with 1:50 (v/v) sequencing grade trypsin (Promega, Madison, WI) overnight (16 hr).
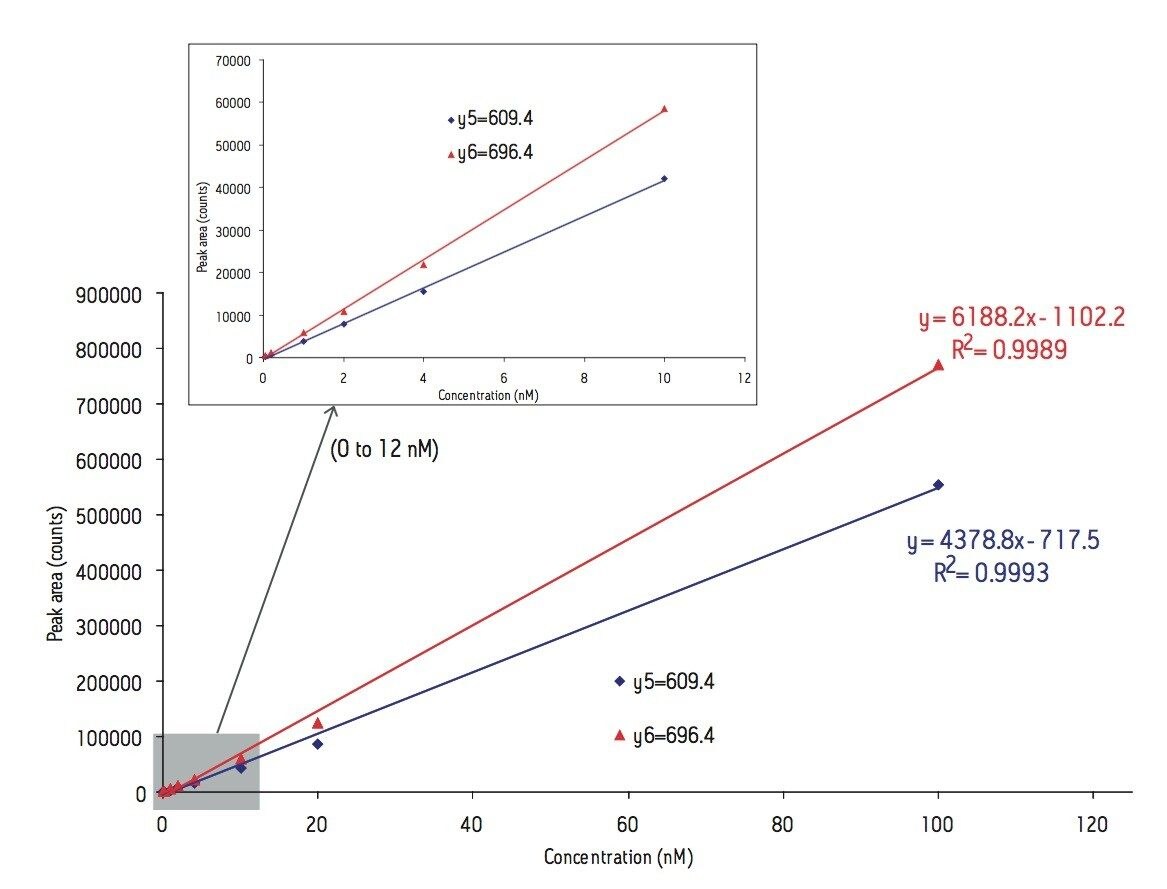
Recombinant C-reactive protein (US Biological, Swampscott, MA) was digested using the same protocol mentioned above and spiked in an undepleteted human serum digest at the concentration of 0.05, 0.2, 1, 2, 4, 10, 20, and 100 nM to build up an external calibration plot for quantitations.
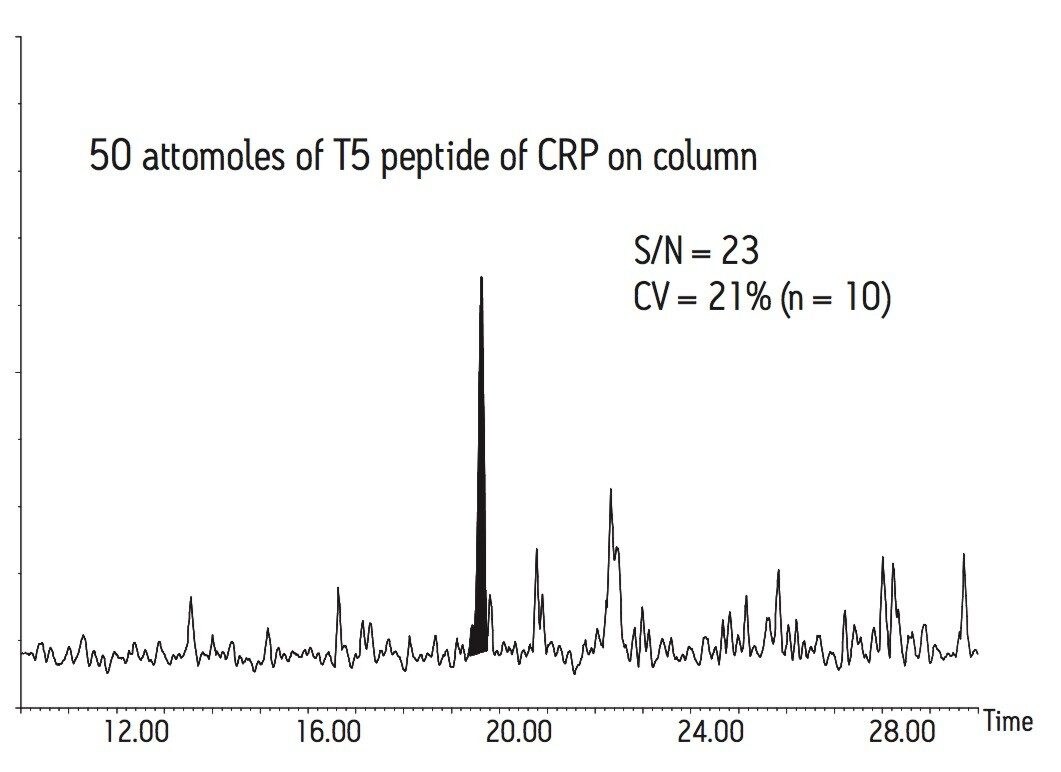
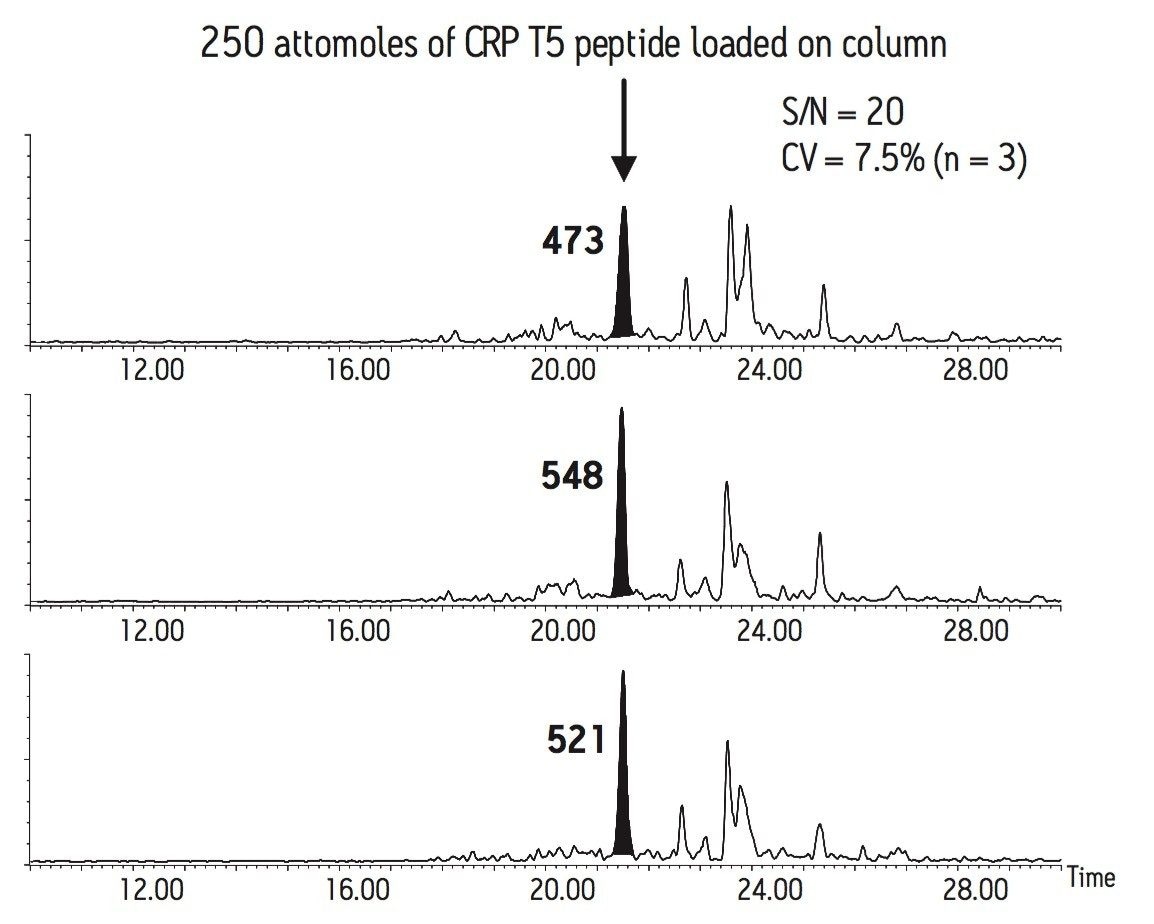
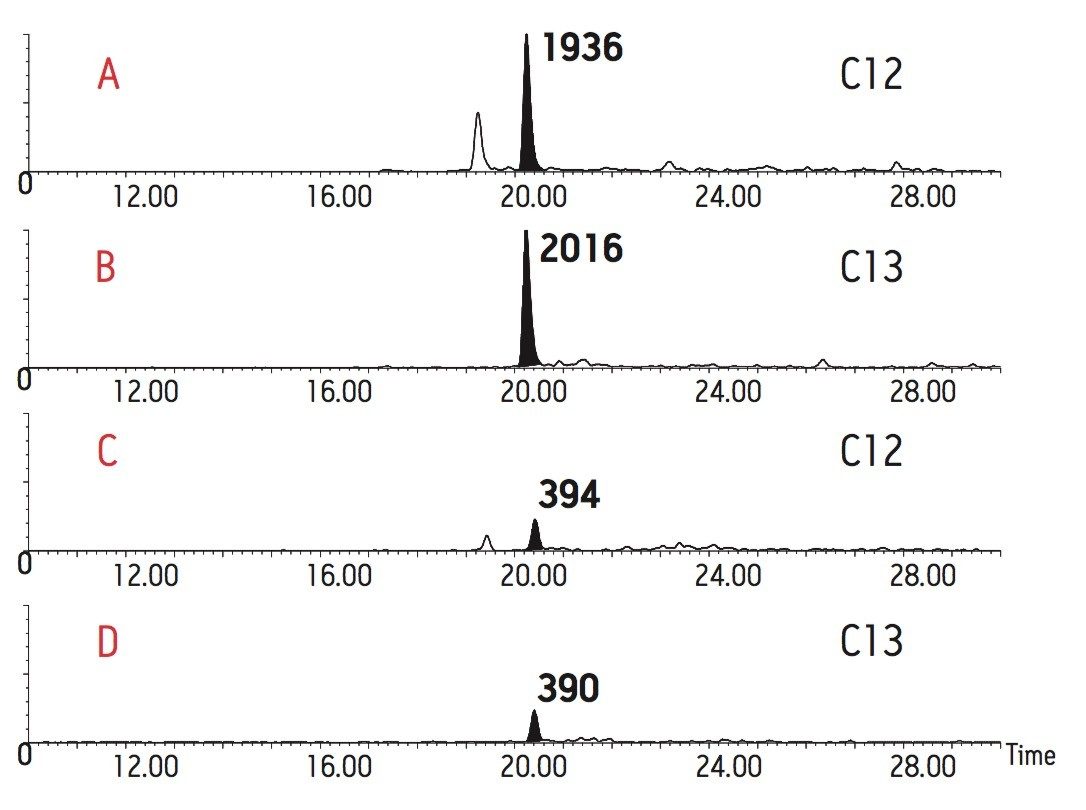
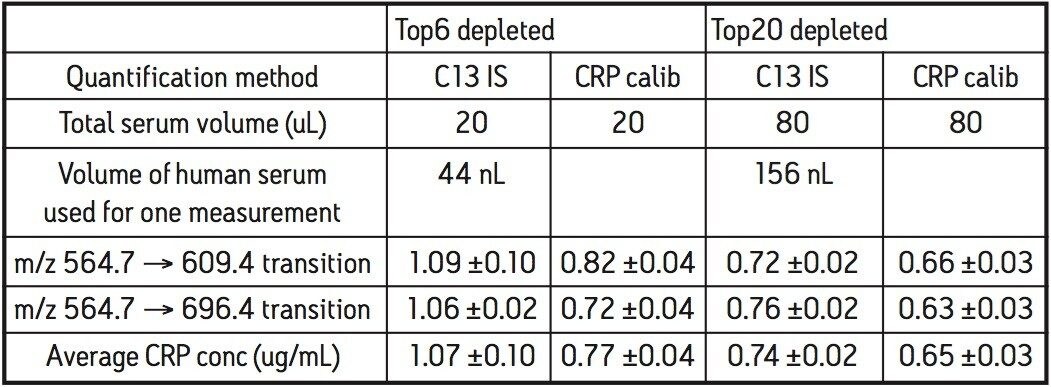
A synthetic peptide containing a 13C-labeled leucine and representing the sequence of T5 peptide from CRP (ESDTSYVSLK) was obtained from New England Peptide (Gardner, MA). It was spiked at two different concentration levels in the Top6 depleted serum digest (0.33 nM) and Top20 depleted serum digest (1 nM).
MRM assays were performed on the nanoACQUITY UPLC System coupled to the Quattro Premier XE Triple Quadrupole instrument.