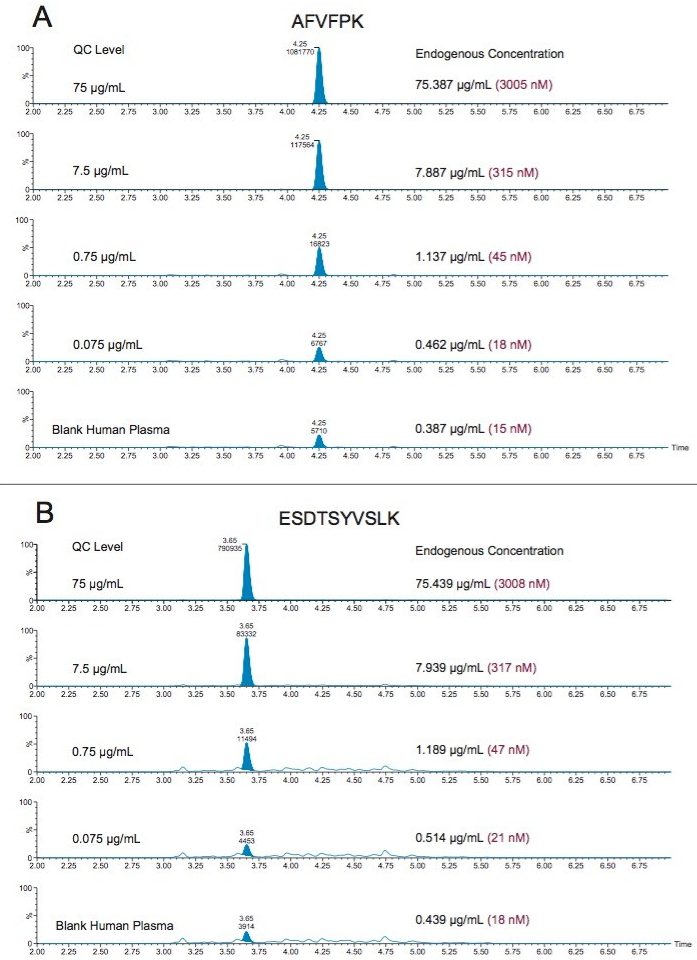
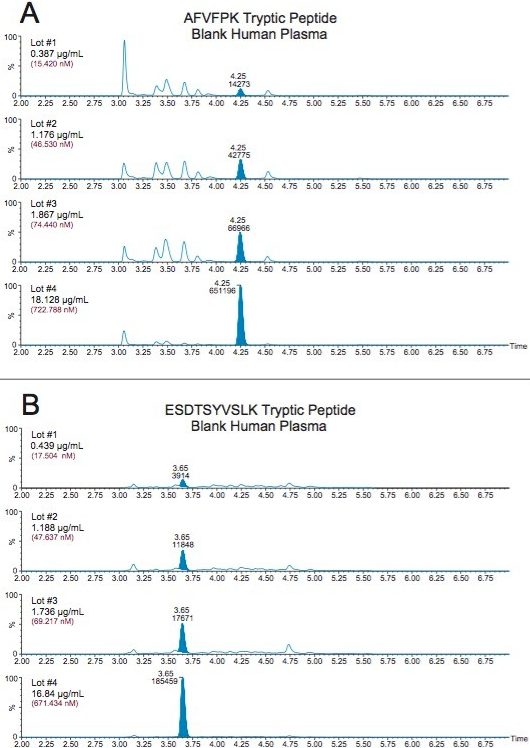
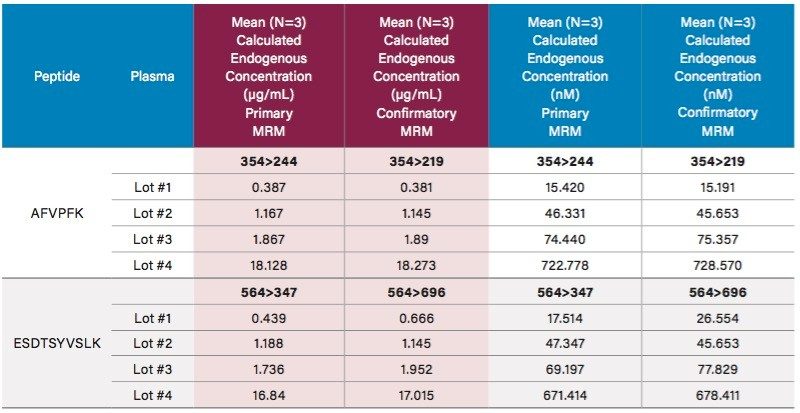
C-Reactive Protein (CRP)1 is naturally synthesized in the liver and released into the bloodstream in response to inflammation. There is, therefore, interest in measuring CRP both in cases of chronic inflammation such as Rheumatoid Arthritis (RA)2,4 as well as to evaluate cardiovascular risk3 and inflammatory cancerous processes.4 Tissue injury or inflammation causes a > 100-fold2 increase in plasma CRP levels. While endogenous plasma levels in healthy individuals are relatively low, generally between 0.1 and 3 µg/mL (4–120 nM),2 levels present in diseased patients are so highly elevated, multiple ELISA or immunoturbidimetric3 tests are required to achieve accurate CRP quantification. The need for multiple tests arises out of the limited linear dynamic range of ligand binding assays (LBA). This inherent short coming, as well as lack of standardization, possible cross-reactivity, and expensive, difficult to reproduce reagents are just a few of the reasons that the industry is moving towards LC-MS. Mass Spectrometry detection offers many benefits for protein quantification such as sensitivity, specificity, broad linear dynamic range, fast method development times, and the ability to multiplex. However, LC-MS protein quantification still presents challenges. There is no single standardized workflow and the various workflow options can be complex and laborious, making it difficult for a scientist to achieve success. In this application note, we describe a generic, kitted approach which requires only 2 hours for digestion vs. a standard 24 hour method described in the literature.5 Digestion and subsequent peptide level purification are performed using the ProteinWorks eXpress Direct Digest (p/n: 176003688) and ProteinWorks µElution SPE Clean-Up Kit (p/n: 186008304) for the accurate and reliable quantification of endogenous CRP in human plasma. The kits and their included protocols achieve LLOQs between 0.025-0.1 µg/mL (1-4 nM) from only 35 µL of plasma.