No significant interferences (recovery within ±15% bias) were observed at the retention time for aldosterone when other structurally related compounds with similar polarities were individually examined (cortisol, cortisone, 18-hydroxycorticosterone, corticosterone, 11-deoxycortisol, 21-deoxycortisol, prednisone, and prednisolone). No significant interference (recovery within ±15% bias) were observed when other endogenous compounds were examined (albumin, bilirubin, uric acid, intralipid, triglycerides, and cholesterol).
No significant system carryover (<20% of the lowest calibrator) was observed from high concentration samples into subsequent blank injections. A 1:5 dilution was successfully employed on high concentration samples, providing a mean accuracy of 100% for aldosterone with an RSD of 2.2%.
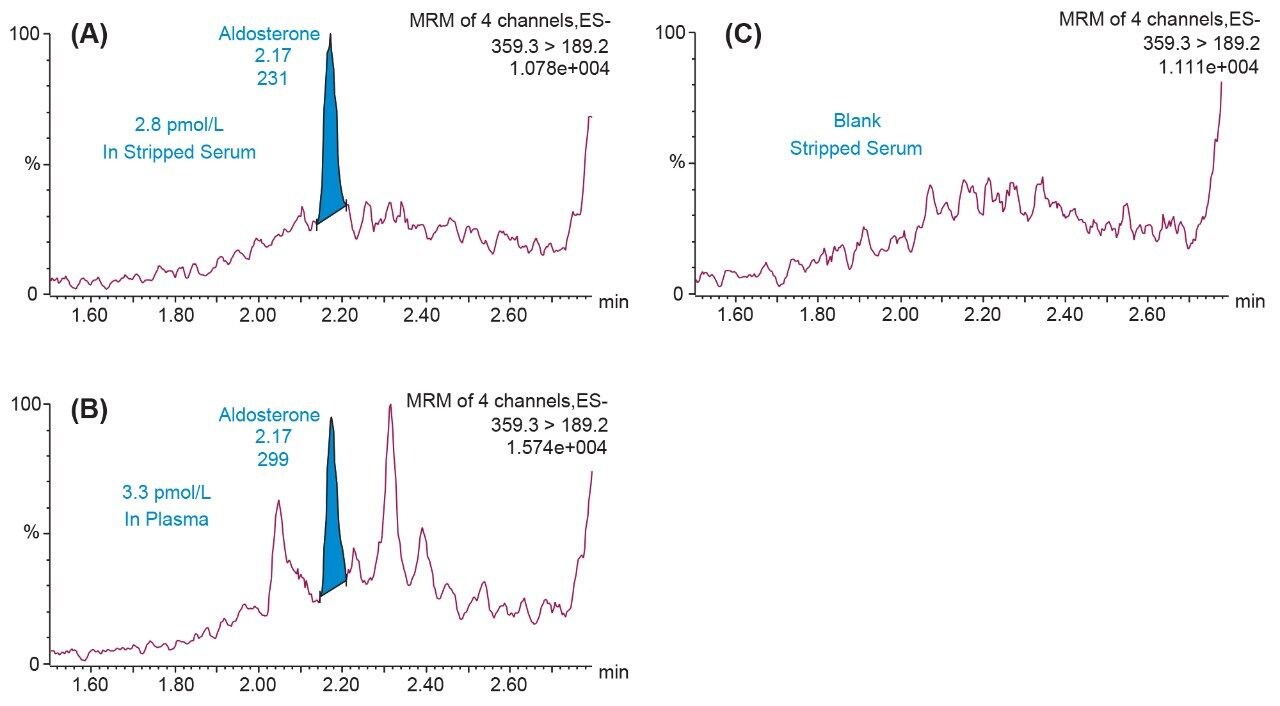
Analytical sensitivity investigations were performed using aldosterone spiked into stripped serum over four occasions across and below the calibration range (n = 40 at each concentration). The method would allow for precise quantification (<20% RSD) at 2.8 pmol/L for aldosterone. The S/N (PtP) was >10 at 8.3 pmol/L.
Total precision was determined by extracting and quantifying five replicates of three level QC material per day over five separate days (n = 25). Repeatability was assessed by analyzing five replicates at each QC level. Low, mid, and high concentrations were 36, 286, and 2932 pmol/L for aldosterone.